 Welcome back to the ThreeSpires Physiotherapy blog and our continuing series of educational articles about issues affecting physiotherapy.In the last blog post I looked at the anatomy of the knee and the structures involved and showed just how complicated the knee is, despite the fact that it is known as just being a relatively simple hinge joint.
Welcome back to the ThreeSpires Physiotherapy blog and our continuing series of educational articles about issues affecting physiotherapy.In the last blog post I looked at the anatomy of the knee and the structures involved and showed just how complicated the knee is, despite the fact that it is known as just being a relatively simple hinge joint.
In this article I thought it might be interesting to try and delve a bit deeper and examine the structures that can cause pain in the knee and look at some of the reasons that they can become painful or a problem and also try to answer the question that, as physiotherapists, we so often hear: "What is wrong with my knee?"
The Collateral Ligaments of the knee
 As described in the previous blog post on the anatomy of the knee, there are two collateral ligaments at the knee joint. The medial collateral ligament (MCL) and the lateral collateral ligament (LCL), these are on the outside of the knee and provide stability and restrict side to side movements.
As described in the previous blog post on the anatomy of the knee, there are two collateral ligaments at the knee joint. The medial collateral ligament (MCL) and the lateral collateral ligament (LCL), these are on the outside of the knee and provide stability and restrict side to side movements.
The MCL is by far the most commonly injured partly because of its attachements to the medial meniscus and mostly because if you have a blow to the knee it is likely to come from the outside and push the knee inwards (as in a tackle in football or rugby). Some form of trauma i.e. a fall, a twist of the knee or a hard tackle is the most common reason for a collateral ligament strain in a sporting environment but it can sometimes be caused by biomechanical weaknesses which we will look into in a bit more detail later.
The Cruciate Ligaments
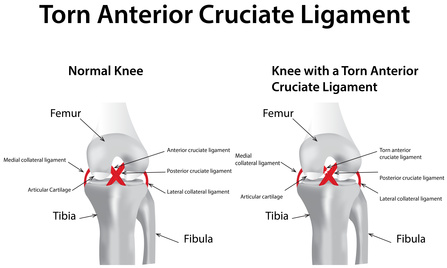 There are two cruciate ligaments inside the knee joint: the anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL), they are both extremely important in terms of stability of the knee and generally if one of your cruciate ligaments is ruptured you will know immediately and there may be a loud pop.
There are two cruciate ligaments inside the knee joint: the anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL), they are both extremely important in terms of stability of the knee and generally if one of your cruciate ligaments is ruptured you will know immediately and there may be a loud pop.
The ACL is by far the most commonly injured and is the most common mechanism is by jumping, then landing and trying to change direction quickly - as is often done by players of many ball sports such as football, hockey and netball.
The PCL is much less commonly injured and it will generally involve the shin being trapped or stopped from moving forward as the femur moves over the top. If you do rupture your ACL there is currently considerable debate as to whether or not it is necessary to repair it surgically immediately or whether it is best to wait and try to strengthen the knee. The answer to this conundrum will depend on how keen you are to avoid surgery, certainly I have seen many patients who have ruptured their ACL did not want surgery and instead worked hard to strengthen and stabilise their knee and now have a strong stable knee that works well without the ligament. On the other hand, if you are playing high level sport and want to return to sport as soon as possible and are happy to have surgery then it is possible that an ACL reconstruction is the right choice for you.
The Menisci of the Knee
Sitting on top of the tibia and in between the femur and the tibia are the menisci, these are semi-circular pieces of fibro-cartilage that perform a vital role in the knee. They are commonly injured and as physiotherapists we see many people with meniscal injuries. They enable the femur to more securely sit on the tibia and improve shock absorption. They are commonly injured in sporting activities and the medial meniscus is often linked with medial collateral ligament injuries due to its link with the MCL. If injured they generally cause pain, swelling and sometimes a locking sensation in the knee and require a thorough assessment by a physiotherapist to determine the next best course of action.
Knee Cartilage
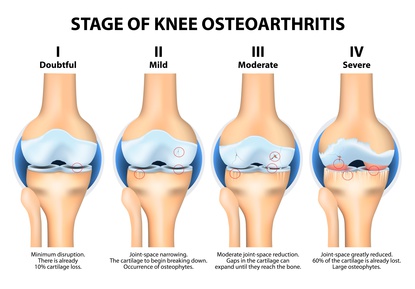 As with every synovial joint in the body the knee joint has cartilage in between the bones such as the tibia, femur and patella. The cartilage is there to reduce friction and improve shock absorption, as we age this cartilage tends to get worn out and what was once a smooth surface becomes pitted and worn.
As with every synovial joint in the body the knee joint has cartilage in between the bones such as the tibia, femur and patella. The cartilage is there to reduce friction and improve shock absorption, as we age this cartilage tends to get worn out and what was once a smooth surface becomes pitted and worn.
If this process continues and advances too far, osteoarthritis will set in - this where the cartilage has become very worn out and the joint has become inflamed. If the process continues further then the cartilage becomes worn away completely and you end up with bone pressing directly on bone which can cause little bony spurs (osteophytes) to develop which cause further pain and inflammation.
The Patella Tendon/Ligament
 The patella tendon extends from the patella (kneecap) to the tibia at what is known as the tibial tuberosity and provides the connection between the quadriceps above and the tibia. As with any ligament or tendon it can become strained and irritated, this usually due to overload or overtraining and can be common in runners who have increased their mileage rapidly.
The patella tendon extends from the patella (kneecap) to the tibia at what is known as the tibial tuberosity and provides the connection between the quadriceps above and the tibia. As with any ligament or tendon it can become strained and irritated, this usually due to overload or overtraining and can be common in runners who have increased their mileage rapidly.
You may have noticed that I have described it as a tendon/ligament and this due to the fact that it can be thought of as both! A tendon connects muscle to bone and a ligament connects bone to bone, however the patella tendon/ligament is an extension of the quadriceps tendon above and the patella is a sesamoid bone which sits inside the tendon. So, depending on your point of view it ether connects the patella to the tibia (and is a ligament) or the patella simply sits inside the whole tendon and it is a tendon!
The Bursae of The Knee
There are several bursae around the knee that can sometimes become inflamed and a source of pain. The most likely culprits in general are the supra-patella bursa, the infra-patella bursa and the pre-patella bursa. If these become irritated as can happen from a large increase in running mileage, a fall onto the patella or an infection then this is known as bursitis.
The Hamstrings and Quadriceps Tendons
At the point the hamstrings (muscles at the back of the knee) and the quadriceps (muscles at the front of the knee) insert into the knee they turn into tendon and as with any tendon they can become strained and inflamed. This often happens due to overload - such as with runners who have increased their training volume to fast. In general patients will feel the pain localised over the particular tendon that is inflamed but sometimes if the person has kept on training it may feel as if the whole knee is sore. As with all injuries the best way to proceed is to seek professional advice from a physiotherapist in order to minimise the long term effects.
In the next blog post we shall take a look at some particular knee pathologies such as patella-femoral pain, Osgood Schlatter's and tendonitis and examine some of the underlying causes for these knee problems. If you or someone you know has knee pain and you would like to understand the cause and how you can improve things then please get in touch. We are a home visit physiotherapy service based in Lichfield and serving surrounding areas such as Sutton Coldfield, Tamworth, Walsall, Rugeley and Burton. We can be contacted on 0788 428 1623 or via email enquiries@threespiresphysiotherapy.co.uk
REQUEST A CALLBACK
Just fill in the form below and give us a quick idea of your problem/request so that we can be better prepared to help you.