 Hello again and welcome back to the ThreeSpiresPhysiotherapy blog. In this post we are going to try and look at what is possibly the most complex joint in the body and answer the question most patients, that see us about their shoulder, have: "Why does my shoulder hurt?" The shoulder is an incredible joint and is certainly the most mobile joint in the human body, it allows the arm to have a huge range of motion, enables the hand to reach way outside our centre of gravity and attaches the arm to the central body and thorax. However, despite being an amazing bit of biomechanical engineering we sometimes ask too much of it....
Hello again and welcome back to the ThreeSpiresPhysiotherapy blog. In this post we are going to try and look at what is possibly the most complex joint in the body and answer the question most patients, that see us about their shoulder, have: "Why does my shoulder hurt?" The shoulder is an incredible joint and is certainly the most mobile joint in the human body, it allows the arm to have a huge range of motion, enables the hand to reach way outside our centre of gravity and attaches the arm to the central body and thorax. However, despite being an amazing bit of biomechanical engineering we sometimes ask too much of it....
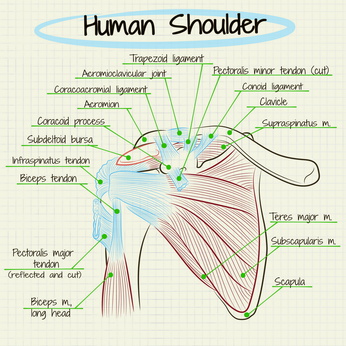
Shoulder pain is extremely common and some studies rate it as the 3rd most common musculoskeletal (MSK) complaint that patients will see a physiotherapist for, certainly our experience at ThreeSpires Physiotherapy has shown it to be extremely common and very frustrating for patients. Before looking at the causes of shoulder pain it could be nice to review the basic anatomy of the shoulder joint as it involves a large number of muscles and some key structures.
 The shoulder joint is a ball and socket joint which is made up of the bones of the humerus (upper arm bone) and scapula (shoulder blade), the head of the humerus (ball part of the joint) articulates with the scapula at the glenoid fossa (this is the socket part of the joint). Although not technically part of the actual shoulder joint (the glenohumeral joint) the clavicle (collar bone) is an important component in attaching the scapula to the thorax (rib cage) and sternum (breast plate). During movement of the arm and shoulder joint as well as the movement at the glenohumeral joint (ball and socket) there is also a large amount of movement from the scapula and the clavicle. As the humerus lifts, in order to support the ball of the head of the humerus, the scapula rotates underneath, as this happens the clavicle also elevates and rotates slightly.
The shoulder joint is a ball and socket joint which is made up of the bones of the humerus (upper arm bone) and scapula (shoulder blade), the head of the humerus (ball part of the joint) articulates with the scapula at the glenoid fossa (this is the socket part of the joint). Although not technically part of the actual shoulder joint (the glenohumeral joint) the clavicle (collar bone) is an important component in attaching the scapula to the thorax (rib cage) and sternum (breast plate). During movement of the arm and shoulder joint as well as the movement at the glenohumeral joint (ball and socket) there is also a large amount of movement from the scapula and the clavicle. As the humerus lifts, in order to support the ball of the head of the humerus, the scapula rotates underneath, as this happens the clavicle also elevates and rotates slightly.
So, that covers the basic bony structures at the shoulder joint: the humerus, scapula and clavicle and how they articulate to create movement at the arm. Now we need to look at some of the other structures around the joint - the ligaments and cartilage which provide passive stability for the joint. Firstly there is the glenoid labrum - this is a piece of fibrocartilage that surrounds the glenoid fossa (the socket part of the joint), this enlarges the socket and increases the overall stability of the joint. It can sometimes get injured during throwing activities and also after shoulder dislocation and physiotherapists often see patients with tears of the labrum (often called SLAP tears), sometimes these patients need surgery and physiotherapy then forms an essential component of the recovery and rehabilitation process..
 Next we have the capsule, which is made up of thick fibres that surround the whole shoulder joint and maintain passive stability of the joint especially at end of range. The anterior (front) portion is much weaker than the posterior and for this reason shoulder dislocation is much more common anteriorly than posteriorly. During the rehab after a shoulder dislocation a comprehensive programme of physiotherapy will be essential to strengthen the shoulder complex and reduce the risk of further dislocations. The shoulder capsule can sometimes be a major source of pain in a condition called adhesive capsulitis (commonly called frozen shoulder) - here the capsule becomes inflamed and extremely painful and slowly movement at the joint becomes impossible.
Next we have the capsule, which is made up of thick fibres that surround the whole shoulder joint and maintain passive stability of the joint especially at end of range. The anterior (front) portion is much weaker than the posterior and for this reason shoulder dislocation is much more common anteriorly than posteriorly. During the rehab after a shoulder dislocation a comprehensive programme of physiotherapy will be essential to strengthen the shoulder complex and reduce the risk of further dislocations. The shoulder capsule can sometimes be a major source of pain in a condition called adhesive capsulitis (commonly called frozen shoulder) - here the capsule becomes inflamed and extremely painful and slowly movement at the joint becomes impossible.
Now we come to the tendons (and by implication the muscles) that insert into the shoulder. For those who have always wondered about the difference between a tendon and ligament it is simply defined as: "a ligament is a piece of connective tissue that connects a bone to a bone" and "a tendon is a piece of connective tissue that connects muscle to bone". The most important tendons of the shoulder are the 4 rotator cuff tendons which insert directly into the head of humerus. These are the most commonly injured structures in the shoulder and some studies say that over 90% of shoulder pain can be attributed to a problem with one of these tendons. These 4 tendons are formed by the 4 rotator cuff muscles: supraspinatus, infraspinatus, subscapularis and teres minor, as suggested by the name "rotator cuff" these muscles are heavily involved with rotation of the arm and shoulder but their major role is that of a stabiliser of the head of humerus (ball part of the joint) - they act as guy lines and suck the head of humerus into the socket. One of these tendons in particular is commonly injured - supraspinatus and is the most commonly injured of the rotator cuff tendons, this is thought to be because it passes through a small gap in the scapula (the subacromial arch) and it can sometimes become compressed and irritated here. Certainly here at ThreeSpires Physiotherapy we see a lot of patients who have injured their rotator cuff and through a programme of exercises targeted at the individual muscles and manual therapy to increase range of motion and reduce pain we see great results. Some patients however may have had a complete tear (rupture) of the tendon and in this case (depending on age and a number of factors) they are likely to require surgery. For these patients physiotherapy to slowly and progressively strengthen the tendon is an essential part of the rehabilitation process.
As well as 4 rotator cuff tendons that insert into the joint there is also another tendon and muscle that can sometimes be implicated as a source of shoulder pain - this is the biceps tendon. Despite being predominantly responsible for elbow flexion the long head of biceps inserts directly into the shoulder joint via the glenoid labrum and can sometimes get overloaded and become a source of shoulder pain. Finally we have the subacromial bursa - a bursa is a fluid/jelly filled sac that reduces friction and in this case sits in between the supraspinatus tendon and the scapula in the subacromial space. A large number of studies have shown it to be heavily innervated (it has lots of nerve endings) and to be a source of shoulder pain. A common orthopaedic procedure that we often see patients after is a subacromial decompression - here the surgeon will take out the bursa and shave off any bone that may be rubbing on the supraspinatus tendon. Again, anyone who has had a subacromial decompression will need a comprehensive programme of physiotherapy to improve range of motion and strengthen and stabilise the shoulder.
Lastly we come to a source of shoulder pain in the more elderly - osteoarthritis, this is where the cartilage in the joint has become worn out and the joint has become irritated. Cartilage is the material in between each bone in any joint in the body that reduces friction and improves shock absorption, as we age the cartilage gets worn down and can become painful. Physiotherapy is usually effective at early management of osteoarthritis in the shoulder and the prevention of worsening of symptoms and if you suspect that you may have osteoarthritis of the shoulder it is important that you get a through assessment to determine how best to manage the condition.
Phew! That is a lot of information and I think it is easy to see why shoulder pain is often extremely frustrating for both patients and physiotherapists alike as there are simply so many structures that can be injured and that may cause pain. In fact it is possible (some would say likely) that there will be more than one source of pain in an injured shoulder. For example with impingement of the supraspinatus tendon there is often an associated irritation of the subacromial bursa making the problem even more difficult to manage.
Physiotherapy can be very successful at reducing shoulder pain and getting patients back to their best and certainly our experience here at ThreeSpires Physiotherapy is that patients who seek advice and treatment earlier have a much shorter recovery time and a generally better prognosis than those who delay for months (and in some cases years!). So if you, or someone you know, would like to know more about how physiotherapy could help with your shoulder then please get in touch: we run a home visit service - seeing anywhere within 25 minutes drive of Lichfield and you can get in touch by phone: 0788 428 1623, email: enquiries@threespiresphysiotherapy.co.ukor us the contact page.
REQUEST A CALLBACK
Just fill in the form below and give us a quick idea of your problem/request so that we can be better prepared to help you.